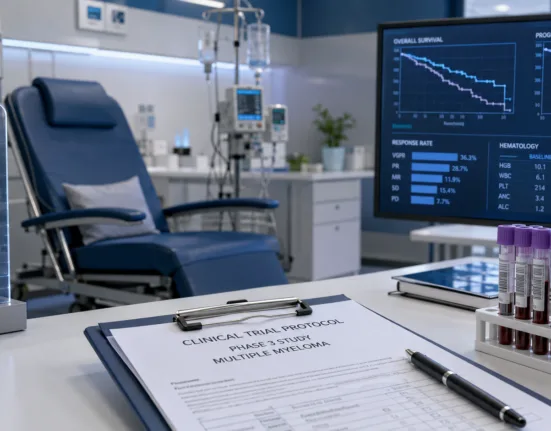
The U.S. Food and Drug Administration has approved Johnson & Johnson’s DARZALEX FASPRO (daratumumab and hyaluronidase-fihj) in combination with bortezomib, lenalidomide, and dexamethasone (D-VRd) for the treatment of adults with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant. The approval was based on the results of the Phase 3 CEPHEUS trial, which demonstrated that the quadruplet regimen significantly improved minimal residual disease (MRD) negativity, deepened response rates, and prolonged progression-free survival versus the standard triplet VRd regimen.
Why MRD-negativity as a primary endpoint could signal a paradigm shift in frontline myeloma trials
This regulatory decision marks a pivotal moment in how clinical success in newly diagnosed multiple myeloma is defined and measured. By anchoring the approval to MRD-negativity as a primary endpoint, the U.S. Food and Drug Administration has effectively validated sustained MRD-negativity as a clinically meaningful surrogate for long-term outcomes. Historically, overall response rate or progression-free survival have dominated as primary efficacy markers. The CEPHEUS trial’s structure—using MRD-negativity at 10^-5 sensitivity and its sustained status over 12 months—signals a growing institutional willingness to prioritize depth and duration of response over traditional endpoints.
Clinicians tracking the evolution of myeloma treatment design believe this endorsement will catalyze broader use of MRD-focused endpoints, particularly in frontline settings where therapy duration, sequencing, and intensity are still evolving. Regulatory watchers note that this sets a precedent not only for CD38-directed antibodies but also for other immunotherapies and bispecifics aiming to displace conventional triplets.
How D-VRd’s depth of response compares with existing regimens in real-world eligible populations
While triplet regimens such as VRd (bortezomib, lenalidomide, dexamethasone) have long served as standard of care for transplant-ineligible patients, the introduction of D-VRd represents a strategic escalation with measurable gains. In CEPHEUS, the MRD-negativity rate at 10^-5 sensitivity was 52.3 percent for D-VRd versus 34.8 percent for VRd. The sustained MRD-negativity over 12 months nearly doubled (42.6 percent versus 25.3 percent), and the hazard ratio for progression or death was reduced by 40 percent (HR 0.60).
However, overall survival data remains immature, which limits definitive conclusions about long-term benefit. Additionally, while D-VRd outperformed VRd across most efficacy endpoints, the trial excluded patients who actively declined transplant, creating a gray zone in real-world generalizability. Clinical uptake may vary depending on institutional tolerance for four-drug regimens in older or frailer populations, especially where supportive infrastructure or monitoring capabilities differ.
Despite these limitations, many hematologists believe D-VRd will become a preferred option in younger, transplant-ineligible patients with preserved functional status. The depth and durability of response, particularly in those with high-risk cytogenetics, may also tip treatment decisions in favor of upfront quadruplets.
Why the subcutaneous formulation of daratumumab matters beyond convenience
One of the strategic advantages of DARZALEX FASPRO is its subcutaneous delivery. This route significantly shortens administration time compared to intravenous daratumumab, with median injection times under 5 minutes and lower rates of infusion-related reactions. That convenience plays directly into real-world adherence, clinic throughput, and overall patient satisfaction. In high-volume community oncology settings, the SC formulation offers logistical efficiencies that facilitate broader deployment of complex regimens like D-VRd.
The co-formulation with Halozyme’s recombinant human hyaluronidase (rHuPH20) underpins this ease of administration. From a payer perspective, subcutaneous options are increasingly attractive due to lower chair time and simplified resource utilization. Johnson & Johnson’s continued migration of DARZALEX usage toward the SC formulation positions it defensively against biosimilar threats and cost-containment pressures, particularly as IV daratumumab faces competition in global markets.
Where D-VRd sits in Janssen’s broader lifecycle strategy for the daratumumab franchise
This approval provides an important lifecycle management lever for Johnson & Johnson. DARZALEX FASPRO now holds twelve total FDA indications, five of which are in newly diagnosed multiple myeloma. The breadth of coverage across transplant eligibility lines consolidates its positioning as the foundational CD38-directed backbone, not just in relapsed/refractory disease but also in first-line care.
Analysts see this milestone as strategic insulation ahead of potential competitors—including next-generation CD38 antibodies, off-the-shelf bispecifics like teclistamab, and pipeline combinations from rivals like Bristol Myers Squibb and Sanofi. The regulatory flexibility shown in approving D-VRd based on MRD outcomes also provides a template for Janssen to push for earlier-line use of novel assets, possibly in fixed-duration strategies or maintenance-free regimens.
Industry observers note that D-VRd also shores up the company’s commercial moat ahead of wider label competition. While isatuximab (Sarclisa) has demonstrated activity in multiple myeloma, it lacks the breadth of indications or the convenience of subcutaneous delivery that DARZALEX FASPRO now offers.
What payers, oncologists, and policymakers will watch post-approval
Despite strong efficacy signals, adoption of D-VRd will hinge on several practical considerations. Reimbursement frameworks will need to reconcile the costs of quadruplet therapy with durability of benefit in older or co-morbid populations. The trial’s exclusion of patients who refused transplant on personal or socioeconomic grounds also limits applicability in underserved communities, potentially introducing new access disparities.
Oncologists are likely to demand real-world evidence tracking long-term functional outcomes, tolerability in multi-morbid patients, and regimen adherence under less controlled conditions. Safety data from CEPHEUS identified common adverse events such as neuropathy, infections, fatigue, and gastrointestinal toxicity—all of which could compromise adherence in community settings. Payors may also look for comparative cost-effectiveness analyses versus fixed-duration regimens or novel agents such as BCMA-targeted bispecifics or CAR-T therapies, especially in resource-constrained systems.
Policy advisors and formulary decision-makers will additionally weigh whether D-VRd improves or complicates treatment sequencing. In an era where salvage therapies are increasingly complex and expensive, using four drugs up front may impact the effectiveness of later lines, particularly if resistance mechanisms or overlapping toxicities emerge.
The strategic horizon: MRD-guided care, fixed-duration trials, and biomarker-defined subgroups
D-VRd’s approval marks more than just an expansion of a product label—it reflects a broader shift in how efficacy is defined, measured, and acted upon in multiple myeloma. If sustained MRD-negativity proves to be a reliable correlate of long-term survival, it could justify time-limited, response-adapted treatment approaches that balance intensity with quality of life.
Janssen’s pipeline may pivot toward MRD-adaptive regimens where therapy is escalated or de-escalated based on serial MRD status. This could dovetail with health system goals around value-based care and reduce long-term toxicity burden. However, regulators and clinicians will likely insist on standardized MRD testing platforms, consistent sensitivity thresholds, and validated correlation with survival before MRD can serve as a universal decision-making tool.
Emerging data may also guide subgroup identification. For example, whether high-risk cytogenetics or early relapsers derive even more pronounced benefit from D-VRd remains an open question. If biomarker-based enrichment becomes viable, it may enable more selective, personalized use of frontline quadruplets.
In sum, while D-VRd is not without limitations, it represents a strong signal that depth of response—measured precisely and sustained meaningfully—is emerging as the new frontier in myeloma care. The industry will now watch to see whether this trial’s success can be mirrored in real-world practice and replicated by future regimens seeking to claim frontline superiority.