Allegheny Health Network has disclosed that cardiac specialists at Allegheny General Hospital successfully performed a transcatheter tricuspid valve replacement using the recently approved EVOQUE Tricuspid Valve Replacement System from Edwards Lifesciences, positioning the institution among the earliest adopters of fully transcatheter therapy for severe tricuspid regurgitation in routine clinical practice. The procedure follows recent United States Food and Drug Administration approval of the EVOQUE system and marks a shift from medical management and repair-only approaches toward definitive valve replacement in a historically underserved structural heart population.
Why full transcatheter replacement for tricuspid regurgitation changes the structural heart playbook
For decades, tricuspid regurgitation has occupied an uncomfortable position in cardiovascular care, widely prevalent, strongly associated with morbidity, yet treated primarily with diuretics and symptom management rather than disease-modifying intervention. Surgical repair or replacement was technically feasible but rarely pursued due to high operative risk, late referrals, and uncertain benefit in a population often burdened by advanced right-sided heart failure.
The transition from repair to replacement via a fully transcatheter approach materially alters that equation. Unlike edge-to-edge repair systems that reduce regurgitant volume but depend on residual native valve anatomy, transcatheter tricuspid valve replacement directly restores unidirectional flow across the valve. Clinicians following the field view this as a more deterministic solution for patients with torrential or complex regurgitation where repair durability is uncertain.

The significance of the Allegheny Health Network case lies less in institutional firsts and more in what it signals about clinical readiness. Transcatheter tricuspid valve replacement is no longer confined to tightly controlled trial environments or elite coastal centers. Its adoption by regional academic hospitals suggests that patient selection criteria, imaging workflows, and procedural safety have matured to a point where broader dissemination is viable.
How the EVOQUE system differentiates replacement from earlier repair-centric strategies
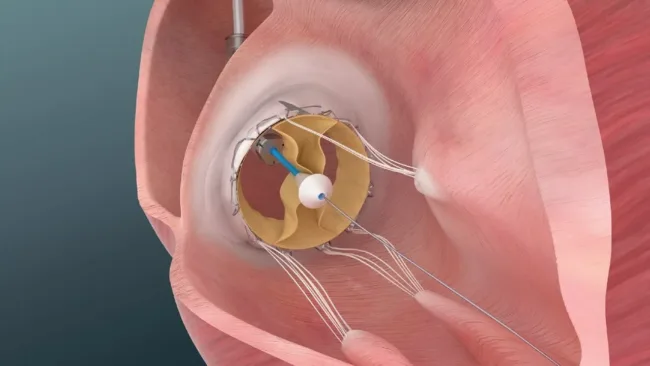
Edwards Lifesciences’ EVOQUE Tricuspid Valve Replacement System represents a deliberate engineering pivot away from incremental repair toward anatomical replacement. The system anchors within the native tricuspid valve via a transfemoral venous approach, expanding to secure position without the need for open surgery or cardiopulmonary bypass.
From a clinical perspective, this matters because tricuspid regurgitation frequently involves severe annular dilation, leaflet tethering, and right ventricular remodeling. These anatomical features often limit the effectiveness of repair devices that rely on leaflet coaptation. Replacement bypasses those constraints by providing a new functional valve, which clinicians believe may translate into more predictable hemodynamic improvement.
Industry observers also note that replacement strategies could simplify procedural decision-making. Rather than debating repair feasibility on a case-by-case anatomical basis, transcatheter replacement offers a clearer pathway for patients previously deemed unsuitable for intervention.
What randomized clinical evidence suggests and what it still does not resolve
The randomized data cited in support of transcatheter tricuspid valve replacement show meaningful improvements in quality of life and functional status compared with optimal medical therapy. Those outcomes are particularly relevant in a condition where mortality endpoints are slow to accrue and symptom burden drives healthcare utilization.
However, regulators and clinicians alike remain cautious about extrapolating early quality-of-life gains into long-term survival benefit. Right ventricular function, interaction with existing pacemaker leads, and long-term valve durability remain open questions that will only be resolved through extended follow-up.
The current evidence base also reflects a relatively selected patient population, typically those with advanced symptomatic disease but preserved enough physiology to tolerate intervention. How replacement performs in earlier-stage tricuspid regurgitation or in patients with severe right ventricular failure remains an active area of debate.
Regulatory clarity exists, but payer interpretation is still evolving
United States Food and Drug Administration approval of the EVOQUE system provides regulatory clarity for clinical use, but reimbursement pathways are still stabilizing. Structural heart interventions often face a lag between approval and uniform payer coverage, particularly for newer indications like isolated tricuspid disease.
Health system executives tracking adoption patterns expect early procedures to concentrate at centers with existing structural heart programs, robust imaging infrastructure, and experience navigating novel reimbursement codes. Over time, as outcomes data accumulate and procedural volumes rise, coverage is likely to normalize, but short-term access disparities are probable.
This dynamic makes the Allegheny Health Network case instructive. Early adoption positions the system to build procedural volume, generate real-world outcomes data, and establish referral pathways before reimbursement becomes fully standardized.
How this shifts referral patterns and clinical behavior
One of the most underappreciated implications of transcatheter tricuspid valve replacement is its potential to change referral timing. Historically, tricuspid regurgitation has been treated as a secondary concern, often addressed only after left-sided disease or when symptoms became refractory.
The availability of a minimally invasive replacement option may prompt earlier referral to structural heart teams, particularly for patients who are symptomatic but not yet in end-stage right heart failure. Clinicians believe that intervening before irreversible right ventricular remodeling could amplify the clinical benefit of replacement therapies.
This shift also places greater emphasis on advanced imaging and multidisciplinary heart teams, as patient selection and procedural planning become central determinants of success.
Competitive implications for the structural heart device landscape
Edwards Lifesciences’ progress in transcatheter tricuspid valve replacement underscores a broader competitive dynamic in structural heart innovation. While multiple companies are pursuing repair-based approaches, replacement platforms offer a distinct value proposition that could ultimately reshape the market.
Industry analysts note that replacement devices may command higher reimbursement and clearer clinical positioning, but they also face higher evidentiary thresholds for durability and safety. As a result, the next phase of competition is likely to center on long-term outcomes, ease of implantation, and compatibility with existing cardiac hardware.
The expansion of replacement into regional centers accelerates this competitive cycle by increasing procedural volumes and generating comparative real-world data.
What could slow adoption despite clinical enthusiasm
Despite growing momentum, several risks could temper adoption. Procedural complexity remains higher than many repair techniques, requiring advanced imaging, operator experience, and careful post-procedure management. Complications related to valve positioning, conduction system interaction, or right ventricular overload remain areas of active surveillance.
Manufacturing scalability and training capacity also matter. As demand grows, device availability and operator training could become bottlenecks, particularly outside major academic centers.
Finally, long-term durability data will be decisive. Structural heart history shows that early enthusiasm can wane if valve performance degrades over time or if unexpected complications emerge in broader populations.
What clinicians, regulators, and industry observers will watch next
The next inflection point for transcatheter tricuspid valve replacement will be longitudinal outcomes. Registries and post-approval studies tracking survival, rehospitalization, and right ventricular remodeling will shape clinical guidelines and reimbursement decisions.
Observers will also watch how replacement competes or coexists with repair technologies. Rather than a binary outcome, the field may stratify patients by anatomy and disease stage, with repair favored earlier and replacement reserved for advanced disease.
For healthcare systems, the question is no longer whether tricuspid regurgitation can be treated interventionally, but how quickly programs can scale expertise to meet latent demand. The Allegheny Health Network case suggests that the era of therapeutic nihilism for tricuspid disease is ending, replaced by a more intervention-forward paradigm.