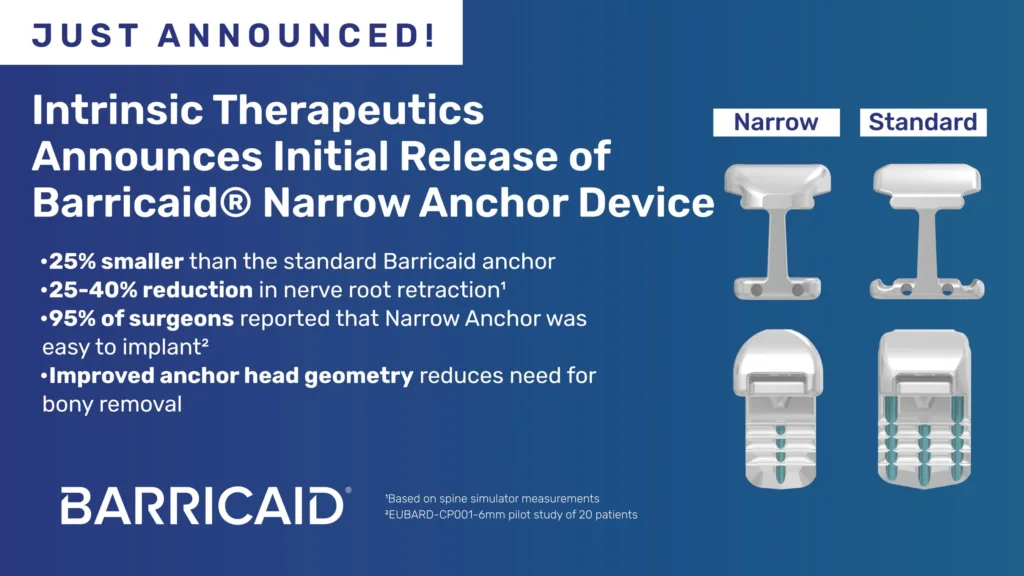
Intrinsic Therapeutics, Inc. has introduced the Barricaid Narrow Anchor, a next-generation version of its bone-anchored annular closure device used after lumbar discectomy. The Boston-based spine technology developer said the updated implant, which is 25 percent smaller than the original Barricaid anchor, is designed to simplify implantation and expand access for patients at high risk of recurrent disc herniation following back surgery.
Why device refinements in annular closure may influence surgical adoption after lumbar discectomy
Lumbar discectomy remains one of the most common surgical treatments for symptomatic disc herniation, particularly when nerve compression leads to severe leg pain or neurological deficits. While the procedure is widely performed and generally effective at relieving symptoms, it carries a persistent challenge. Recurrence of disc herniation at the operated level remains one of the most frequent complications.
Industry observers note that reherniation rates following discectomy can range from roughly 5 percent to more than 20 percent depending on patient characteristics and defect size in the annulus fibrosus, the outer wall of the intervertebral disc. Large annular defects, in particular, have been associated with significantly higher recurrence rates.
Annular closure devices emerged as a strategy to address this structural weakness. By physically sealing the defect left after disc material removal, these implants aim to prevent residual disc fragments from escaping through the annular opening. Intrinsic Therapeutics developed the Barricaid platform to anchor a polymer mesh to the adjacent vertebral bone, creating a barrier at the defect site.
The release of the Narrow Anchor variant reflects a shift toward surgical usability rather than a fundamental redesign of the therapy itself. In spine surgery, incremental improvements that simplify implantation can influence adoption patterns. Surgeons frequently weigh device complexity, procedure time, and learning curve alongside clinical performance when deciding whether to incorporate a new technology into routine practice.
What the narrower Barricaid anchor reveals about procedural challenges in spine surgery
According to Intrinsic Therapeutics, the new anchor reduces the bone anchor width from 8 millimeters to 6 millimeters. That reduction may appear minor, but within the confined anatomy of the spinal canal it can have meaningful procedural implications.
Spine surgeons must often retract nerve roots during implantation of devices placed near the intervertebral disc space. Excessive retraction can increase the risk of nerve irritation or postoperative pain. Simulator testing cited by the manufacturer suggests that the narrower anchor can reduce nerve root retraction by between 25 percent and 40 percent during implantation.
Clinicians tracking the field suggest that even small ergonomic improvements can influence procedural safety and efficiency. In minimally invasive spine procedures, limited visualization and tight anatomical corridors create challenges for surgeons placing implants. A smaller anchor may therefore allow easier positioning while preserving the mechanical fixation needed to secure the device.
Improved visualization during placement is another element highlighted in the redesign. Optimized anchor geometry reportedly improves the surgeon’s view of the implant during insertion. For surgeons adopting annular closure devices, this type of procedural feedback can play a role in determining whether the technology fits seamlessly into existing surgical workflows.
What clinical evidence supporting the Barricaid platform suggests about long-term outcomes
The Barricaid system has been supported by multiple clinical investigations over the past decade. Intrinsic Therapeutics reports that the device has been implanted in nearly 13,000 patients globally. Published research includes randomized controlled trials and observational studies evaluating recurrence risk following lumbar discectomy.
A multicenter randomized controlled trial published in the Journal of the American Medical Association compared outcomes between patients undergoing discectomy alone and those receiving discectomy with Barricaid implantation. That trial focused on patients with large annular defects, a subgroup known to face elevated recurrence risk.
Five-year follow-up data from the study suggested that annular closure significantly reduced rates of reherniation and reoperation compared with discectomy alone. Industry observers often cite this trial as one of the stronger evidence bases supporting the use of annular closure devices.
However, clinicians emphasize that clinical outcomes depend heavily on patient selection. Annular closure devices are typically recommended only for patients with specific defect characteristics following disc removal. Surgeons must evaluate annular defect size and other anatomical factors before determining whether the device is appropriate.
The introduction of the Narrow Anchor does not appear to change the fundamental clinical indication for the Barricaid platform. Instead, it represents an engineering refinement designed to maintain the same mechanical stability while reducing surgical complexity.
Why reimbursement signals from the American Medical Association may matter for adoption
Beyond device design, reimbursement pathways often determine whether surgical technologies gain widespread traction. Intrinsic Therapeutics highlighted the inclusion of a dedicated Current Procedural Terminology code for bone-anchored annular closure in the American Medical Association’s 2026 CPT Code Set.
The code, which took effect in January 2026, provides a standardized billing mechanism for the procedure. Health economists note that reimbursement clarity can remove a significant barrier to adoption for hospitals and surgeons.
In many cases, new surgical devices struggle to gain traction not because of clinical limitations but because of reimbursement uncertainty. Without clear procedural coding, hospitals may hesitate to adopt technologies that could complicate billing or reimbursement.
The addition of a CPT code does not guarantee widespread payer coverage, but it does represent an important milestone in the commercial lifecycle of a surgical innovation. Regulators, insurers, and hospital administrators will likely monitor utilization patterns as the procedure becomes more formally recognized within reimbursement frameworks.
How annular closure fits within the broader spine surgery technology landscape
The spine surgery device market has historically evolved through a series of incremental innovations rather than sudden breakthroughs. Technologies such as intervertebral cages, artificial discs, and minimally invasive instrumentation have gradually reshaped surgical practice over decades.
Annular closure devices occupy a more specialized niche within this ecosystem. Their primary goal is not to replace existing procedures but to improve outcomes for specific high-risk patient groups.
Some surgeons remain cautious about adopting additional implants in procedures that are already effective for many patients. Discectomy alone continues to deliver strong outcomes for a large proportion of individuals with disc herniation.
At the same time, clinicians treating recurrent disc herniation recognize the clinical and economic burden of repeat surgeries. Revision procedures often involve greater complexity, longer recovery times, and higher healthcare costs.
For this reason, technologies that reduce recurrence risk may appeal to surgeons managing patients with large annular defects or other recurrence risk factors. Observers suggest that improved procedural simplicity, such as that offered by the Narrow Anchor, may help expand the pool of surgeons willing to evaluate annular closure as part of their surgical toolkit.
What clinicians and regulators are likely to watch as the Barricaid platform evolves
As with many surgical implants, long-term data and real-world outcomes will continue to shape the trajectory of the Barricaid platform. Registries and post-market surveillance studies may provide additional insight into complication rates, device durability, and patient outcomes across diverse surgical settings.
Regulatory watchers also tend to monitor how device modifications affect performance. Even relatively small design changes must maintain the safety and mechanical reliability established by earlier versions.
Intrinsic Therapeutics reports that the Narrow Anchor passed the same mechanical testing standards applied to the original device, including resistance to anchor migration and structural fracture. Maintaining these characteristics is essential for implants placed within the spinal column, where mechanical stability is critical.
Clinicians tracking the field also emphasize the importance of surgeon training. Annular closure procedures require familiarity with patient selection criteria and implantation techniques. If the new design reduces the learning curve associated with the procedure, adoption could gradually increase.
Another factor to watch is the broader evolution of spine surgery toward minimally invasive approaches. Devices that integrate smoothly with minimally invasive surgical techniques may hold an advantage in operating rooms increasingly focused on reducing tissue disruption and shortening recovery times.
What the Barricaid Narrow Anchor launch ultimately signals about the spine device market
The introduction of the Barricaid Narrow Anchor reflects a familiar pattern in medical device innovation. Once a technology demonstrates clinical viability, manufacturers often shift attention toward improving usability, expanding indications, and strengthening reimbursement pathways.
Rather than transforming the annular closure concept itself, the updated anchor highlights the role of surgical ergonomics in determining whether a device becomes widely adopted. For many surgeons, practical considerations such as implantation ease and procedural efficiency carry as much weight as clinical performance data.
Industry observers suggest that the long-term success of annular closure devices will depend on several interconnected factors. These include continued evidence demonstrating reduced recurrence rates, reimbursement clarity, and the ability to integrate seamlessly into modern spine surgery workflows.
The Barricaid Narrow Anchor therefore represents a step in the gradual maturation of the annular closure category. Whether it ultimately accelerates adoption will depend on how surgeons, hospitals, and insurers interpret the growing body of clinical and economic evidence surrounding the technology.
Intrinsic Therapeutics introduces Barricaid Narrow Anchor as surgeons seek better reherniation prevention tools added by Pallavi Madhiraju on
View all posts by Pallavi Madhiraju →