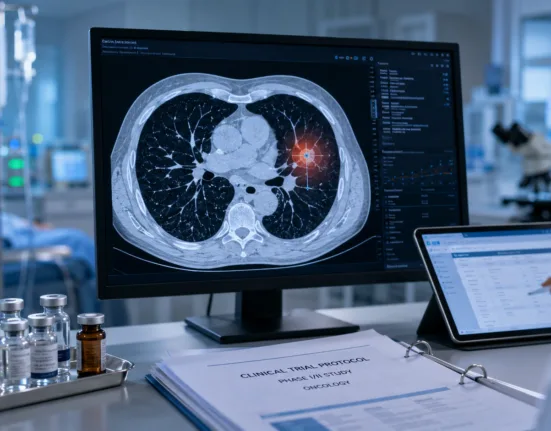
Personalis, Inc. has reported pivotal findings from its NeXT Personal assay in a new Cell publication, highlighting the test’s ability to detect molecular residual disease in stage I to III non-small cell lung cancer. The study, part of the TRACERx initiative and led by Professor Charles Swanton of the Francis Crick Institute and University College London, followed 431 patients for more than five years. It confirmed that the NeXT Personal assay identified circulating tumor DNA at levels that not only preceded radiologic relapse by months or even years, but also predicted relapse risk and overall survival outcomes with high sensitivity.
What the TRACERx results reveal about the limitations of imaging in lung cancer follow-up
The extended follow-up and volume of patients in the TRACERx cohort provided a rare opportunity to track the performance of an ultra-sensitive, tumor-informed ctDNA assay across diagnosis, treatment, and surveillance. With relapse still a leading cause of mortality in early-stage NSCLC, the study underscores a major limitation of the current standard of care: reliance on imaging to confirm disease progression or recurrence. Personalis’ ctDNA platform detected relapse between 5 to 9 months earlier than radiographic scans in the median case, and in some instances, up to 57 months ahead.
This diagnostic gap is especially problematic given the window of opportunity that often exists post-surgery and during adjuvant therapy. As adjuvant immune checkpoint inhibitors and chemotherapy regimens become more complex, the need to know who is relapsing earlier—and who is not benefiting from treatment—is increasingly urgent. The NeXT Personal test introduces a possible inflection point in lung cancer care, allowing for more nuanced post-operative risk stratification and potentially reducing the likelihood of overtreatment in molecularly negative patients.
Why NeXT Personal’s detection threshold changes the clinical utility equation
What differentiates NeXT Personal from other MRD assays is its ability to detect ctDNA at approximately 1 part per million, made possible through whole-genome sequencing combined with proprietary error correction and noise suppression algorithms. This capability proved crucial in identifying a specific subset of patients with ultrasensitive but non-zero ctDNA levels, who fell into an intermediate-risk group. While traditional imaging would consider these patients disease-free, the assay revealed an elevated likelihood of future relapse and worse overall survival outcomes.
This stratification power matters because NSCLC relapse trajectories are often heterogeneous. Some patients remain disease-free for years after surgery, while others experience rapid recurrence despite therapy. The ability to detect even faint traces of ctDNA redefines what clinicians consider a “clean margin” after resection, and could reframe the decision-making process around surveillance intensity and extended therapy options.
How this study positions Personalis among ctDNA and MRD competitors
Personalis now enters a competitive liquid biopsy landscape alongside players like Guardant Health, Natera, and Foundation Medicine, all of whom are advancing their own ctDNA and MRD platforms for solid tumors. However, most competing assays offer either fixed-panel or limited hybrid-capture approaches, often optimized for high-burden metastatic disease. By contrast, NeXT Personal is designed for low-burden, early-stage applications—a niche where high specificity and low false-negative rates are paramount.
The company’s decision to publish in Cell—following other peer-reviewed validations in Nature Medicine and Annals of Oncology—signals a strategy to anchor clinical credibility before pursuing broader commercial deployment. The TRACERx dataset also bolsters confidence, given its independent academic leadership and large-scale, longitudinal structure. That combination gives Personalis an edge in demonstrating real-world assay reliability, especially in a space where false reassurance from underperforming MRD assays could have serious consequences.
What remains unclear about adoption and regulatory pathway
Despite the strength of the data, Personalis will face a series of hurdles on the path to clinical integration. One immediate question is whether the U.S. Food and Drug Administration will treat NeXT Personal as a laboratory-developed test or require full regulatory clearance as a companion diagnostic. The assay’s performance in the TRACERx study could support the latter, but formal regulatory submissions are likely still pending.
In parallel, payers will demand clear evidence of clinical utility. While the study showed prognostic correlations between ctDNA detection and relapse, it did not establish that using the test to guide therapy alters patient outcomes. To achieve reimbursement, Personalis will likely need prospective interventional trials where treatment is adjusted based on assay results—either escalation for ctDNA-positive patients or de-escalation for ctDNA-negative individuals. Until those data arrive, widespread clinical adoption may remain limited to academic or self-pay settings.
Why clinicians are cautiously optimistic—but not yet fully aligned
Clinicians familiar with MRD testing in hematologic malignancies may welcome the NeXT Personal approach, but oncologists in solid tumors are likely to proceed more cautiously. One challenge is the interpretation of ultrasensitive positive results, which can be difficult to act upon in the absence of radiologic confirmation. There is also the risk of false positives from clonal hematopoiesis, although Personalis’ tumor-informed design may mitigate that.
Moreover, not all ctDNA assays yield equivalent results. Variability in panel design, sequencing depth, and error suppression can significantly influence both false-negative and false-positive rates. As a result, lung cancer experts will look for independent validations across multiple tumor types and diverse clinical settings before embracing the assay in routine practice. Ongoing studies or registries that track outcomes in real-world deployments could help build that confidence.
What this could mean for MRD testing beyond lung cancer
While TRACERx focused specifically on NSCLC, the implications of this publication extend to other early-stage solid tumors where relapse detection is often delayed. Cancers such as colorectal, bladder, and triple-negative breast cancer are among the likeliest next targets for ultra-sensitive MRD testing, given the high relapse burden and limited utility of imaging post-therapy.
Personalis’ broader pipeline suggests an ambition to develop pan-tumor residual disease surveillance tools that can adapt across cancer types. Success in NSCLC could set the stage for regulatory submissions in other indications, particularly if the company can demonstrate similar performance metrics and clinical relevance. The strategy echoes broader industry trends toward modular, tumor-informed diagnostics that can be customized for multiple settings with minimal infrastructure change.
Where this positions Personalis strategically in 2026 and beyond
If Personalis can capitalize on the TRACERx publication, the company may redefine the competitive dynamics of the MRD and liquid biopsy sector. Its whole-genome approach and emphasis on longitudinal monitoring could complement existing diagnostic pipelines, enabling partnerships with drug developers and oncology networks. The technology could also serve as a pharmacodynamic biomarker in trials for adjuvant therapies or immuno-oncology agents, helping identify early non-responders and refine dosing strategies.
However, the path to commercial success will depend on a combination of regulatory clarity, payer acceptance, and clinician education. Demonstrating cost-effectiveness, workflow integration, and actionable insights in prospective clinical trials will be key milestones. With relapse prediction timelines extending into multi-year lead times, the company’s long-term value proposition may be strongest in settings where early intervention translates into tangible survival or quality-of-life benefits.