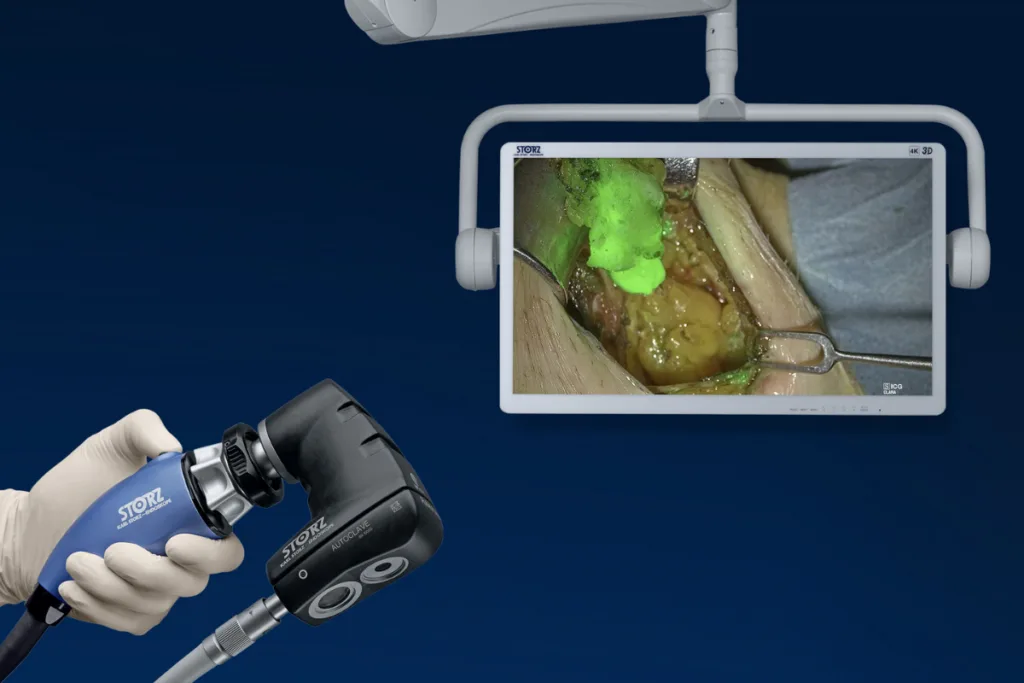
KARL STORZ has received FDA clearance for the Rubina Lens exoscope for open surgery, extending its near-infrared and indocyanine green fluorescence imaging ecosystem across open and minimally invasive procedures in the United States. The clearance gives surgeons a digital, camera-based 4K exoscope designed to support real-time tissue perfusion assessment, lymphatic mapping, and breast surgery where fluorescence imaging may assist intraoperative decision-making.
Why does the Rubina Lens clearance matter for open surgery visualization strategy?
The regulatory clearance matters less because fluorescence imaging is new and more because KARL STORZ is moving an established visualization concept into a broader open surgery setting. Near-infrared imaging with indocyanine green has already become familiar across several surgical workflows, particularly where clinicians need additional visual cues on perfusion, lymphatics, vessels, or tissue boundaries. The gap has often been consistency across surgical approaches, since hospitals may use different imaging configurations for laparoscopic, robotic, microscopic, and open procedures.
That is the strategic significance of the Rubina Lens clearance. KARL STORZ is not only offering another imaging device, it is attempting to reduce the separation between open and minimally invasive visualization infrastructure. For hospitals that already use KARL STORZ imaging towers, the appeal is likely to be continuity rather than reinvention. Surgical teams may be able to bring fluorescence-guided visualization into open procedures while staying within a familiar operating room architecture, monitor-based workflow, and imaging ecosystem.
The limitation is equally important. This is a visualization clearance, not a clinical outcomes claim. The device can help surgeons see information that may not be visible under standard white light, but adoption will still depend on whether surgical teams believe that additional fluorescence information changes intraoperative decisions often enough to justify training, workflow integration, and device utilization. In open surgery, where experienced surgeons are already accustomed to direct visual and tactile assessment, the bar for changing routine practice can be quietly high.
What is genuinely new and what remains incremental in KARL STORZ’s fluorescence imaging expansion?
The genuinely new element is the United States clearance for the Rubina Lens exoscope in open surgery, which extends KARL STORZ’s near-infrared and indocyanine green imaging footprint beyond fully endoscopic workflows. The device combines a wide-angle exoscopic view with white-light and fluorescence visualization, giving surgeons a monitor-based view of the surgical field and the option to switch into near-infrared imaging when indocyanine green is used in line with its approved labeling.
The incremental element is that the clearance builds on already cleared components, existing imaging infrastructure, and the broader clinical familiarity of indocyanine green fluorescence. The FDA pathway also reflects that posture. The KARL STORZ ICG Imaging System with Rubina Lens System was cleared through a traditional 510(k) submission based on substantial equivalence to predicate devices, supported by comparative bench testing and performance evaluation rather than a new prospective clinical trial. That makes the device commercially meaningful, but not disruptive in the way a first-in-class device or a trial-backed outcomes technology would be.
This distinction matters for clinicians and procurement teams. A technology that is incremental can still be valuable if it lowers adoption friction, improves consistency, and fits existing capital equipment. However, incremental devices can also struggle if hospitals view them as nice-to-have enhancements rather than essential workflow tools. KARL STORZ’s task is therefore not just to demonstrate image quality, but to show that the Rubina Lens improves operating room efficiency, surgeon confidence, and case-to-case usability in ways that matter to service line leaders.
How could near-infrared and indocyanine green imaging influence tissue perfusion and lymphatic mapping?
The clinical relevance of the Rubina Lens sits in the areas where visual uncertainty can influence intraoperative choices. Tissue perfusion assessment can be relevant in plastic, microvascular, and reconstructive surgery, where surgeons may need additional cues on blood flow and tissue-transfer circulation. Lymphatic visualization and lymph node delineation can be relevant in procedures where mapping is part of intraoperative management, including breast surgery.
In those contexts, fluorescence imaging does not replace surgical judgment. It adds another layer of visual information that can help support decisions around perfusion, lymphatic pathways, and the visibility of structures that are not adequately assessed by the naked eye alone. The device’s wide-angle view and monitor display could be useful in open surgery because the surgical field is not constrained by a laparoscopic view, while the ability to use the exoscope handheld or on a holding arm gives teams flexibility across different procedure types and operating room layouts.
The unresolved question is how consistently that added visual information changes the decision pathway. A clearer fluorescence signal may support confidence, but the device’s value will vary by procedure, surgeon preference, indocyanine green protocol, timing of administration, lighting conditions, field depth, and team familiarity. Industry observers are likely to watch whether the technology becomes concentrated in high-value reconstructive and breast surgery use cases or spreads across a broader range of open procedures.
Why could integration with existing KARL STORZ platforms be commercially important for hospitals?
The commercial logic of the clearance rests heavily on platform integration. The Rubina Lens is designed to work within the KARL STORZ ICG Imaging System and related IMAGE1 S Rubina infrastructure, which means the medical device manufacturer can position the product as an expansion of existing fluorescence capability rather than a wholly separate capital purchase. That matters in hospitals where equipment committees are under pressure to justify spending against staffing constraints, margin pressure, and competing requests from surgical departments.
For installed-base hospitals, the practical pitch is straightforward. If the operating room already uses compatible KARL STORZ imaging infrastructure, adding open surgery fluorescence capability may look more like extending a platform than creating a new technology silo. That can reduce friction around training, service support, procurement review, and standardization. In a market where hospitals increasingly prefer interoperable systems and vendor consolidation, that is not a small advantage.
The risk is that integration is only attractive where the installed base is already strong. Hospitals using competing fluorescence imaging systems, robotic imaging platforms, or handheld perfusion assessment devices may not see the same upgrade logic. In mixed-vendor environments, Rubina Lens will need to compete not only on image performance, but also on footprint, ease of setup, sterility workflow, reprocessing requirements, service economics, and the perceived burden of adding another device to the operating room.
What does the FDA pathway reveal about the strengths and limits of the clearance?
The FDA clearance provides a clear regulatory route into the United States market, but it also frames the device as a substantial-equivalence product rather than a technology supported by new clinical outcome data. The 510(k) summary identifies the system as a Class II device and describes comparative bench testing, optical performance testing, near-infrared and indocyanine green imaging performance evaluation, and safety assessments as the basis for the submission. Clinical testing was not required because the device was found to have the same intended use and similar technological characteristics as predicate devices.
That pathway is common and appropriate for many medical devices, especially when the technology builds on established categories. For hospitals, it gives regulatory confidence that the device can be marketed for its cleared indications. For clinicians, however, it does not answer every adoption question. Bench testing can support safety and performance, but it does not prove that the device improves surgical outcomes, reduces complications, shortens procedure time, or lowers readmission rates in real-world open surgery.
This is where market development becomes important. KARL STORZ may need clinical education, procedure-specific evidence, and surgeon-led use cases to convert clearance into routine utilization. The company does not need to prove a drug-like efficacy endpoint to sell the device, but it will need to help hospitals understand where fluorescence imaging changes decisions and where it merely adds another screen to an already complex operating room.
How does Rubina Lens fit into the broader competition around fluorescence-guided surgery?
Rubina Lens enters a field where fluorescence-guided surgery has become an increasingly important battleground across endoscopy, robotics, open imaging, and handheld devices. The competitive landscape includes systems that emphasize portability, robotic integration, laparoscopic compatibility, high-definition visualization, or procedure-specific workflow. KARL STORZ’s advantage is likely to come from ecosystem breadth rather than a single isolated feature.
The medical device manufacturer can now tell a more complete visualization story across minimally invasive and open surgery. That is strategically useful because surgical departments do not always think in technology categories. They think in procedure lists, physician preference cards, training requirements, service contracts, and equipment availability. A fluorescence system that can follow more procedures across more settings may become easier to standardize.
The counterpressure is that open surgery does not automatically behave like minimally invasive surgery from a technology adoption standpoint. In laparoscopy, the camera is central to the procedure. In open surgery, imaging is an adjunct layered on top of direct access to the field. That means Rubina Lens must prove that monitor-based exoscopic fluorescence adds enough value without slowing setup, disrupting surgeon ergonomics, or creating dependency on a display when direct visualization remains available.
What are the adoption and reimbursement questions hospitals may ask next?
Hospitals are likely to examine the Rubina Lens through a practical economic lens. The absence of a need for a wholly separate imaging platform could help adoption where compatible KARL STORZ systems are already present. Still, reimbursement for surgical imaging tools is rarely simple. Hospitals may not receive a distinct premium merely because fluorescence visualization was available during a case, so the business case may need to come from standardization, procedure efficiency, reduced uncertainty, or support for higher-acuity surgical programs.
Training will also matter. Near-infrared and indocyanine green imaging depends on understanding when to use the dye, how to interpret fluorescence, and how to avoid overreliance on image signal. The imaging output can be valuable, but it is not a binary answer machine. Signal intensity, timing, tissue thickness, field conditions, and camera distance can all affect interpretation. That makes education and procedural discipline essential, especially when the technology moves into open surgery environments with varied setups.
The operational question is whether surgical teams will find the device easy enough to use repeatedly. A device that is technically strong but awkward to position, clean, schedule, or integrate into case flow may see limited utilization. The Rubina Lens can be used handheld or mounted, which gives flexibility, but flexibility can also introduce variation. Hospitals will likely want clear protocols on when the device is used, who sets it up, how imaging modes are selected, and how findings are documented.
What should clinicians, regulators, and medical device observers watch after clearance?
Clinicians should watch whether Rubina Lens use clusters around specific procedures where fluorescence information is already valued, such as reconstructive surgery, tissue perfusion assessment, lymphatic mapping, and breast surgery. Early adoption in focused use cases would be more meaningful than broad but shallow marketing claims across every open procedure. In surgical imaging, durable adoption usually follows clear procedural value, not general-purpose capability.
Regulators and safety observers may focus on post-market experience, particularly because open surgery exoscopes combine illumination, camera positioning, sterile-field interaction, and fluorescence imaging. Any device used near tissue for prolonged periods must be managed carefully, especially where light source intensity, distance, setup, and operator handling can influence safety. The 510(k) testing framework addresses performance and safety requirements, but real-world use will still depend on proper training and adherence to instructions.
For the medical device sector, the broader signal is that fluorescence-guided surgery is continuing to move from specialized capability toward platform feature. KARL STORZ’s clearance suggests that the next phase of competition may be less about whether near-infrared imaging works and more about which companies can make it routine, flexible, and economically acceptable across the widest range of surgical environments. That is a quieter contest than headline-grabbing robotics, but for hospitals trying to standardize operating room technology, it may prove just as consequential.





